This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solveb those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Case:
This is a case of a 35 year old male with chief complaints of loss of sensation in both limbs below knee and upper limbs below elbows since 6 months.
Daily routine- patient is a labourer by occupation.
He wakes up in the morning at 6 am
Has his breakfast (rice)by 8am
Goes to work at 9am
Has his lunch at 1pm
He goes back home by 8pm
Patient has been drinking alcohol since he was 15 years old.He has a habit of drinking throughout the day.
He also chews tobacco.
History of presenting illness:
Patient was apparently asymptomatic 4 years back. He then developed stomach pain where he got admitted to hospital when he got diagnosed as having high blood sugar as an incidental finding and started on oral hypoglycemic drugs then since 6 months he stopped taking medications for
diabetes from then he develop polyphagia, polydypsia
increased frequency of urination present
delayed wound healing present weight loss present
Tingling sensation of both upper & lower limbs present
Loss of sensation present
Numbness present
No Burning micturition
Loss & sensation initially present in B/L feet which progressed to below knees since he stopped medication
Past history:
K/C/o DM since 4 years -Stopped Medication since 6 months due to financial constraints
Not a k/C/O HTN,TB, CAD, Asthma, epilepsy
Personal history:
Diet: mixed
Apetite: decreased
Bowel and bladder: increased frequency
Addictions: alcohol since he was 15 years old
GENERAL EXAMINATION:
Patient is conscious,coherent and cooperative, moderately built and moderately nourished.
Pallor: absent
Icterus: absent
Cyanosis: absent
Clubbing: absent
Lymphadenopathy: absent
Pedal edema: absent
VITALS:
Temperature: 98 degree farenheit
Pulse: 90 beats/minute
Blood pressure:120/80mm Hg
Respiratory rate: 20 cpm
SYSTEMIC EXAMINATION:
CVS: S1 and S2 are heard
RS: bilateral air entry present
Abdomen: soft and non tender
CNS: higher mental functions intact
Right. Left
Reflexes: biceps. +. +
Triceps. +. +
Supinator. +. +
Knee. +. +
Ankle. + +
Plantar Flexion. Mute
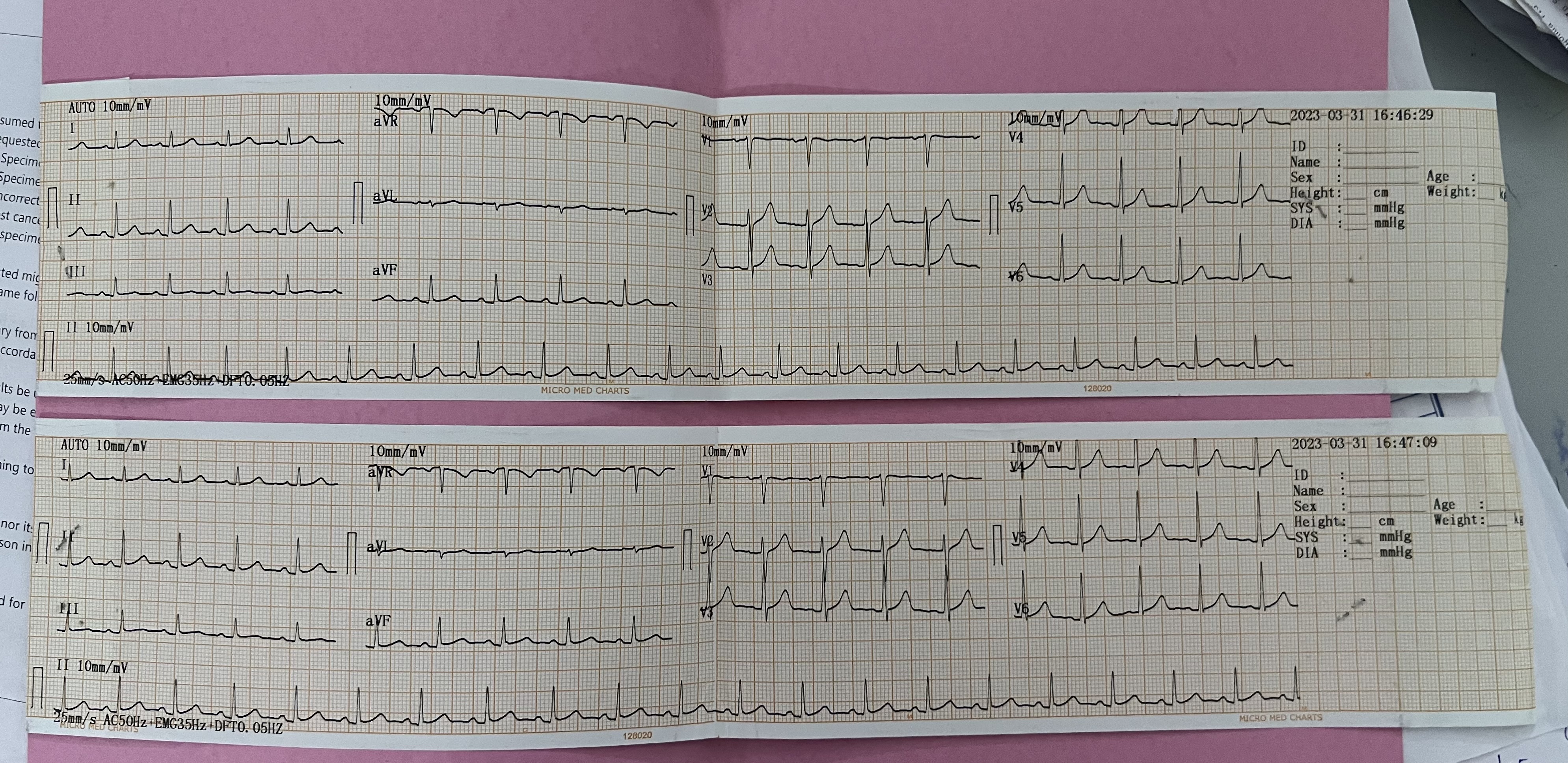
Investigations:
Provisional Diagnosis:
Uncontrolled sugar secondary to non compliance to OHA
Alcohol dependence syndrome and tobacco dependence syndrome
Diabetic polyneuropathy
Treatment:
1) IV 1) IV Fluids NS @ 75 mIl he
2) INJ THIAmINE 200mg in l00M, NIS
8Am -28m - 8Pm
3) INS OPTINEUROM in 100ML





















Comments
Post a Comment