A 30 year old female with chest pain and pain in the right lumbar
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solveb those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
CASE:
A 30 year old female came with chief complaints of
-Chest pain since 2 years
- Pain in the right lumbar region since 6 months
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic 2 years ago.She complained of chest pain (substernal region)which was insidious in onset.Initially 2 years ago,pain was present only during the day but at present the pain is present during day and aggravates at night.
Pain is radiating to the back (interscapular region) and is intermittent,dragging in nature and tenderness on touch.
Each episode lasting for 15-20 mins during the day and it gets aggravated during the night everyday while lying down on bed or while bending down.
It relieves spontaneously.
She complained of pain and tenderness in the right lumbar region which is intermittent (4-5 times a week) since 6 months.It aggravates after she has spicy and oily food.
It is of prickly and burning type of pain which is associated with bloating,nausea,headache and dizziness for which she takes pantop for temporary relief.
She has belching and bitter after taste.
She also complained of black colour stools 4-5 episodes since 6 months.
DAILY ROUTINE:
Patient wakes up by 8am in the morning.She is a home maker and makes breakfast for the family.
She has tea,biscuit and roti for breakfast.
She does her daily chores and has lunch by 2pm (rice and vegetables).
She takes a nap for 1-2 hours.
In the evening she looks after her child’s studies and makes dinner by 10pm.
She goes to bed at 11pm.
PAST HISTORY:
Patient is not a known case of HTN,DM,Asthma,Epilepsy,Tuberculosis and thyroid abnormalities.
PERSONAL HISTORY:
Sleep:Normal
Apetite: decreased since 6 months
Diet: mixed
Bowel and bladder: regular
Addictions: paan, (supari) areca nuts daily since 3-4 years.
FAMILY HISTORY:
No similar complaints in the family.
GENERAL EXAMINATION:
Patient is conscious,coherent and cooperative, moderately built and moderately nourished.
Pallor: mild pallor
Icterus: absent
Cyanosis: absent
Clubbing: absent
Lymphadenopathy: absent
Pedal edema: absent
VITALS:
Temperature: 98 degree farenheit
Pulse: 92 beats/minute
Blood pressure:120/70mm Hg
Respiratory rate: 18 cpm
SYSTEMIC EXAMINATION:
CVS: S1 and S2 are heard
Respiratory: bilateral vesicular breath sounds are present
CNS: no focal neurological deficits
Abdomen: soft and tenderness is present only when there is pain






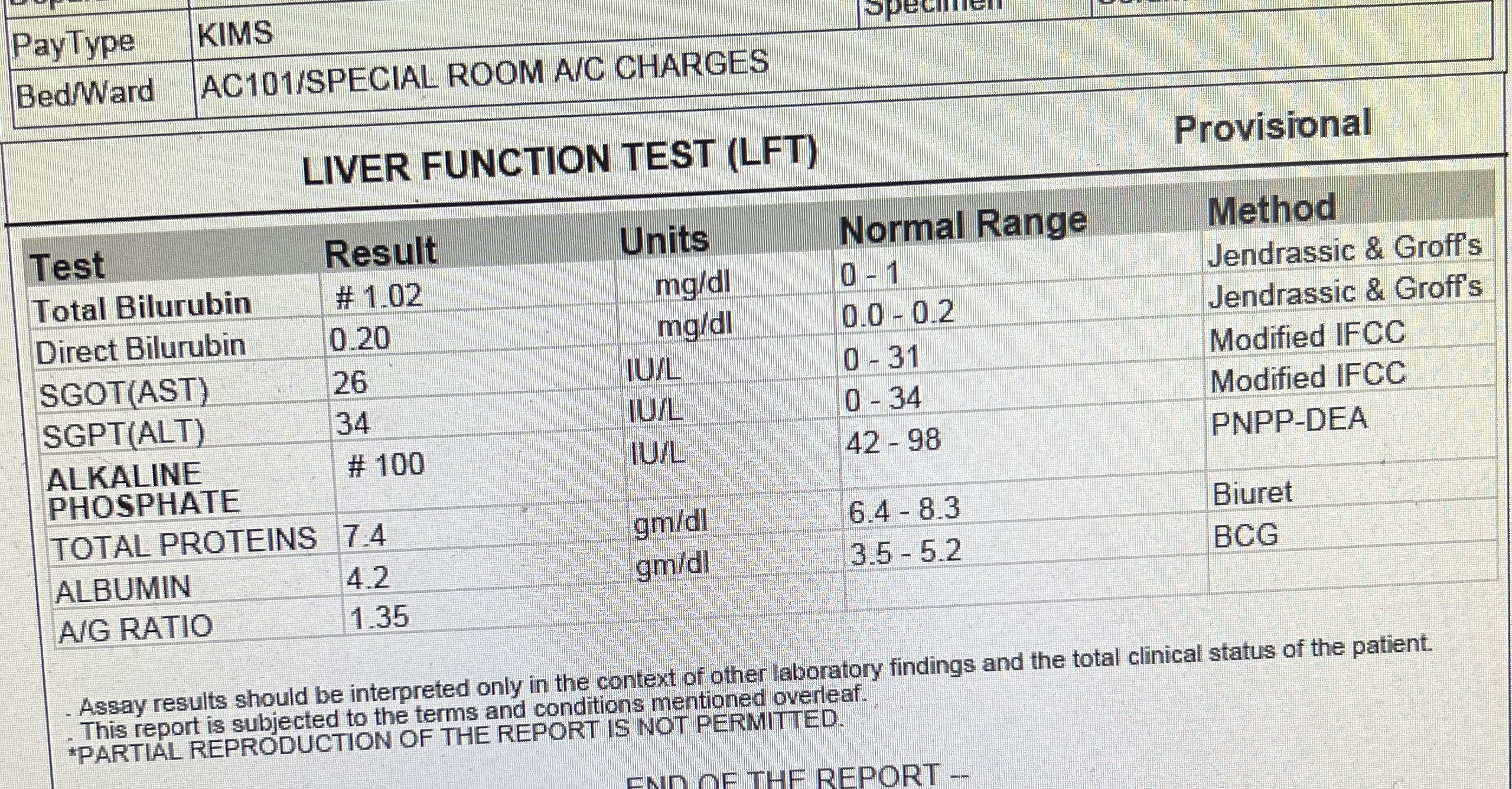
INVESTIGATIONS:



Ultrasound report:


X ray:


PROVISIONAL DIAGNOSIS:
Chronic gastritis
TREATMENT:
Tab Pantop 40mg PO/OD
Tab Brufen 400mg PO/BD



Comments
Post a Comment