A 58 year old male with fever,vomitings,decreased apetite,decreased urine output since 15 days
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solveb those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
A 58 year old male came with chief complaints of
-fever since 15 days
-decreased apetite since 15 days
-decreased urine output since 15 days
-vomitings since 10 days
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic 16 days back. He went to another hospital where he complained of decreased micturation, shortness of breath (grade 4).He was then referred to here.
He then developed high grade fever which was continuous and not relieved by medication.
He complained of vomitings since 10 days which occurs immediately after having food,non bilious and one episode of blood stained of vomiting.
He also complained of burning micturation and decreased urine output since 15 days.
DAILY ROUTINE:
He wakes up in the morning around 6-7 am. He has his tea and breakfast. He stays at home all day and watches tv. In the evening he does beedi and drinks alcohol with friends.He skips dinner when he drinks alcohol.At night he sleeps around 7-8 pm.
PAST HISTORY:
Not a known case of HTN,asthma,epilepsy
Patient is a known case of diabetes mellitus since 10 years
He had a history of Tuberculosis 20 years ago for which he had taken medication for 9 months.
10 years ago, he developed lower limb weakness for which he was taken to the hospital.The physician had told him that he has low levels of sodium and potassium.He was diagnosed with diabetes at the same time. He was given medication.
Since then he stopped going to work (occupation: farmer).
PERSONAL HISTORY:
Sleep: decreased
Diet:mixed
Apetite: reduced
Addictions: alcohol since 30 years and smokes beedi since 30 years
(1 pack a day).
GENERAL EXAMINATION:
Pallor: absent
Icterus: absent
Cyanosis: absent
Clubbing: absent
Lymphadenopathy: absent
Pedal edema: absent
VITALS:
Temperature: 98.4 degree farenheit
Pulse: 79 bpm
Respiratory rate: 16 cpm
Blood pressure: 100/70 mm hg
SpO2: 96%
SYSTEMIC EXAMINATION:
CVS:S1 and S2 are heard
Respiratory: bilateral vesicular breath sounds are presents
CNS: no focal neurological deficits
Abdomen: soft and non tender
shape of abdomen: scaphoid

INVESTIGATIONS:
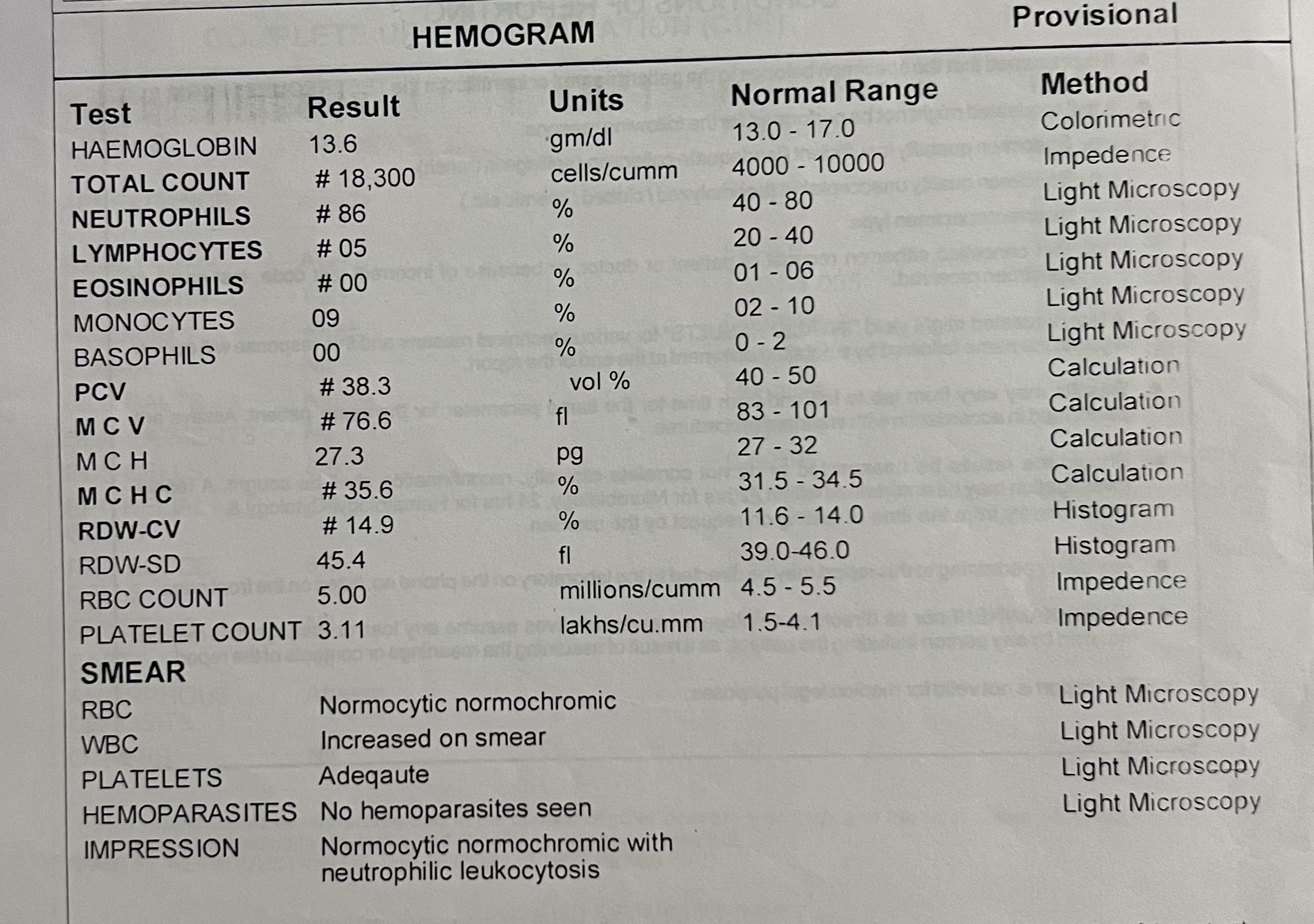




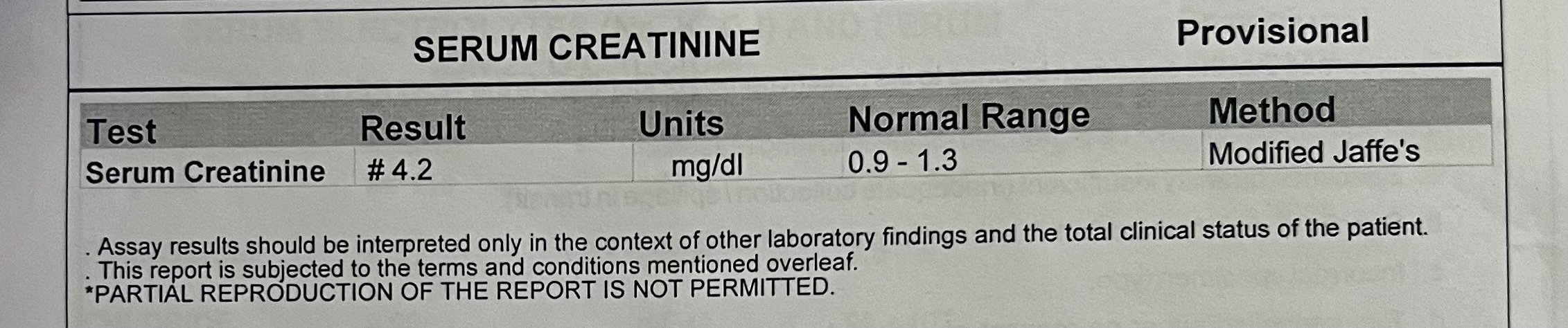







PROVISIONAL DIAGNOSIS:
AKI on CRF secondary to diabetic nephropathy
Old Kochs
H/o hypokalemic periodic paralysis
TREATMENT:
Inj. Piptaz 2.25gm TID
Inj. NS infusion 10ml/hour
Inj. Pan 40mg iv OD
Inj.Lasix 20 mg BD
Inj. Neomol



Comments
Post a Comment